 Primary Care Network Vision for a Resilient Medicines Safety Culture – Ethical Considerations for Commissioners and Providers October 2019 Dr Liliana Risi
Primary Care Network Vision for a Resilient Medicines Safety Culture – Ethical Considerations for Commissioners and Providers October 2019 Dr Liliana Risi
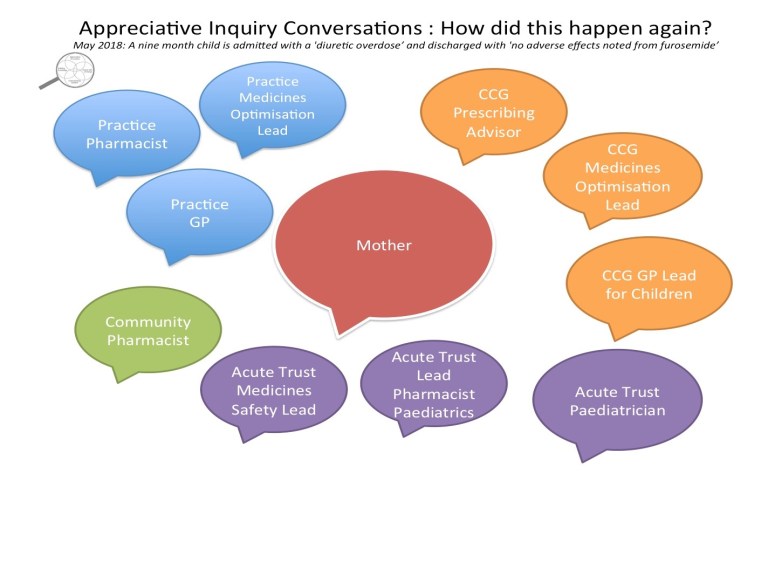
“Every system is perfectly designed to get the results it gets.”
In May 2018 a nine-month child was accidently given an overdose of furosemide by his mother. An appreciative enquiry approach was used to process map this incident. Conversations with everyone involved revealed opportunities to prevent the error, as the risks of using different formulations of the same medicine in primary and secondary care were already well known. This raised the question about current methods for capturing and learning from medicines harms. The purpose of this paper is to demonstrate, using the improvement science lens, that there is already information in the system available to help commissioners and providers minimise medication errors. Instead of introducing new methods of capturing medication errors or technical strategies to improve safety, which have balancing effects on the system, rather what is needed is a shift to strengthening human factors and relationship based learning. Primary care networks are an ideal opportunity to test system learning from significant events through multi-disciplinary reflective learning with commissioners so that the World Health Organization (WHO) challenge to every health system to halve severe and avoidable harm caused by medicines by 2022, can be achieved.
Published by handyapproachtocare

Currently (April 2025) I work as a Humanist Chaplain in an Acute East London NHS Hospital Trust, hold the role as the Non-Executive Director for Greener Practice and am an Associate with the QMUL Medical School Flourishing Team.
I have held roles in the RCGP and am Emeritus Provost of the RCGP North East London Faculty . I was Provost from 2019 to 2022 and responsible for Leadership, Scholarship and Fellowship. Prior to this I was Chair from 2016 to 2019 and Treasurer from 2014 to 2016.
I have an interest in trauma transformed care and creative climate health creation. I have co-facilitated the London Deep End Health Equity Leadership platform growing leaders for fairer systems and healthier places.
The published work informing this web page can be found here: The Handy Approach – Quick Integrated Person-Centred Support Preparation
I am committed to #healthierhealthcare which is about the delivery of proportionate, respectful, and equitable care.
More about me here in the Lancet 2004: https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(05)66406-9/fulltext
You can find me on @lilianarisi.bsky.social View all posts by handyapproachtocare

